tarsal tunnel syndrome
AUTHOR: Marc Mitnick DPM home --> tarsal tunnelWHAT IS A TARSAL TUNNEL
Tarsal Tunnel Syndrome is the compression of the main nerve (posterior tibial nerve) that passes under the medial or inside part of the ankle. Peripheral nerves such as the nerves in the feet are richly endowed with their own blood supply and have the ability to stretch or shorten along with the movement of the accompanying joint; in this case the ankle joint.
When the nerve is entrapped in its tunnel the swelling that occurs around the nerve and the ensuing scarring of the nerve inhibit blood flow to the nerve. As the ankle joint continues to move the nerve is further compressed and the ability of the nerve to properly function is diminished.
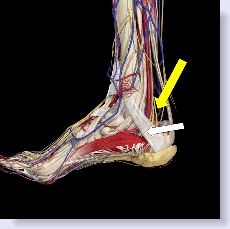
tarsal tunnel anatomy
The tarsal tunnel location is on the inside portion of the ankle, just below the medial malleolus, (the bone on the inside of the ankle.)
Below is an anatomical diagram of the band, known as the laciniate ligament represented by the white arrow pressing against the nerve, while the yellow arrow is pointing to the nerve itself.
|
what causes tarsal tunnel
Causes of this syndrome include trauma such as a fall, acute or chronic pronation of the foot that creates excessive pressure on the inside of the ankle. Additionally, a tendonitis of the tendon that passes through the tunnel can create similar symptoms because as the tendon swells it creates excessive pressure within the confined area putting pressure on the nerve. A
Below is an example of pronation. See how the arch has collapsed. This creates excessive tension on the inside of the ankle thus causing pressure on the nerve.
|
tarsal tunnel pain
Symptoms include burning or numbness usually on the bottom of the foot. It may be worse when standing or walking. There may also be muscle weakness of the muscles that run through the bottom of the foot. The distribution of pain or numbness is dependent on which nerve branch of the posterior tibial nerve is most affected. For that reason all of the foot or only certain parts of the foot may be affected.
Diagnosis is made by the history of the pain or numbness in the area of the distribution of the nerves on the bottom of the foot. Tenderness may be noted over the nerve just behind the ankle joint. Tapping with a finger may send sensations both forward into the foot and backward up the leg; this is known as a positive Tinel's sign. Your foot specialist should be able to determine the distribution of numbness with simple tests. There may also be muscle weakness particularly in the inability to bend your toes in a downward fashion.
Your foot specialist may also order an electromyogram (EMG) which may reveal decreased nerve conduction across the tarsal tunnel. If your doctor feels there may be a soft tissue mass, he may order an MRI.
tarsal tunnel test
The Kinoshita test is a pronatory "stress test". Your doctor may attempt to bend your foot upwards and at the same time pronate the foot. The foot is held in that position for ten seconds. At this point, if you have tarsal tunnel syndrome, you will start to feel the symptoms. This test was developed in 2002 and in the initial study after the patients went on to have surgery, the effectiveness of the test was confirmed in 42 out of 43 feet.
Other foot conditions may mimic the symptoms of this condition. These may include radiculopathy (nerve impingement in lower back), diabetic neuropathy, peripheral neuropathy, rheumatoid arthritis, vascular disease, Baxter's nerve (heel neuroma), plantar fasciitis, scar tissue from previous trauma or surgery, ankle edema (swelling) and possibly a growth like a ganglion cyst, or lipoma (fat tumor) in the canal.
HOW DO YOU TREAT TARSAL TUNNEL SYNDROME
orthotics for tarsal tunnel syndrome
Treatments include the use of orthotics when the origin of the problem appears to be excessive pronation.An orthotic will prevent the foot from over pronating and thus relieve the pressure on the nerve. Click here for a discussion of tarsal tunnel and orthotics.
If the origin of the problem is traumatic in nature, a tarsal tunnel brace may be indicated as the brace or in many instances, a walking cast, will prevent the ankle from moving at all and will allow the inflammation in the tarsal tunnel to subside.
Adding a heel lift to the walking cast can be helpful as the slight plantarflexion that is created also helps reduce the tension and pressure on the affected nerves.
Along with the above treatments your foot specialist may also prescribe oral anti-inflammatory medicine to help reduce the inflammation.
A tarsal tunnel injection of corticosteroid may also be beneficial.
Transcutaneous nerve stimulation may be helpful as a supplemental treatment as long as the underlying cause of the tarsal tunnel is being addressed.
tarsal tunnel exercises and home remedies
Other then trying an orthotic that you may purchase, there is very little you can do to remedy your symptoms. Additionally, there are no exercises which will help and actually too much exercise may aggravate your symptoms.
If none of the conservative avenues work then you must consider surgical intervention. Aside from the existing symptoms, if the pressure is not removed from the nerve, the nerve will eventually fail all together making it almost impossible to walk. The surgery itself is a soft tissue procedure whereby the ligament band pressing on the nerve is incised; the posterior tibial nerve is freed from all constricting bands. This is an out-patient procedure. You will usually require a walking cast. However, prior to consenting to surgery other causes of these symptoms should be ruled out. These include diabetic neuropathy, a pinched nerve in the lower spine, alcoholism, rheumatoid arthritis and heavy metal neuritis just to name a few.
TARSAL TUNNEL RELEASE PROCEDURE
This is a soft tissue procedure that can be performed on an out patient basis. An incision is made just underneath the inside of the ankle bone. The laciniate ligament is a ligament that binds or holds all the vessels and nerves as they pass under the ankle joint. This ligament is incised in an effort to release the pressure that is pressing on the posterior tibial nerve which is causing the tarsal tunnel symptoms.
In addition to releasing the ligament, the area is inspected for the possibility of a growth such as a ganglion cyst which may also be causing pressure on the posterior tibial nerve. Any adhesions (fibrotic tissue attached to the nerve) is also dissected away thus freeing up the nerve.
The skin is closed. The patient may or may not be placed in a walking cast based on the preference of the surgeon.
REFERENCES
The New England Journal of Medicine
The American Journal of Medicine

|

|

|
Want more information? CLICK HERE
Para traducir esta pagina, ve al boton de traduccion de Google en las esquina superior derecha de la pagina
Specific Recommendations For This Condition
KLM ORTHOTICS
In my opinion, the best pre-made orthotic available. Offers the best combination of support and cushioning. Will work in the greatest percentage of people who try a pre-made orthotic. (keep in mind, everyone's foot structure is different and so unlike a prescription orthotic, pre-made devices can be hit or miss). In order to treat capsulitis, this orthotic has to be ordered with a metatarsal pad. Click the link below for a full description.
REDITHOTICS
Many of you are forced to wear dress shoes on a daily basis and it can be difficult to get an orthotic into a dress shoe since there is limited space. Redithotics are a pre-made orthotic designed specifically for this purpose. In order to treat capsulitis, this orthotic has to be ordered with a metatarsal pad. Click the link below for a full description.


Recent Articles
-
Vitamin D impact on health
Feb 06, 23 07:17 PM
Researchers are suggesting that the effectiveness of Vitamin D in fighting and preventing disease is predicated on a persons body mass index (BMI). The thinner the person the greater the positive impa… -
Foods to speed up healing
Feb 01, 23 02:41 PM
One of the best ways to help yourself heal faster after surgery is to eat well. Getting the proper nutrition will provide your body with the essentials it needs to promote healing. Here is a suggestio… -
Cancer and Type 2 Diabetes
Jan 25, 23 04:52 PM
An article revealing that older type 2 diabetics have a higher incidence of cancer then non-diabetics. It is suggested that cancer may surpass CVD as the number one cause of death in older diabetics. -
Does glucosamine or MSM reduce arthritis pain?
Jan 22, 23 01:41 PM
A good review of the possible benefits to taking glucosamine, chondroitin or MSM for arthritis. Always beware of the possible side effects of over the counter supplements. -
shin splints
Jan 18, 23 05:12 PM
A great review on the various causes of shin splints, along with treatment options. -
Whats new in skin cancer?
Jan 15, 23 08:32 PM
A presentation of newer skin protection combinations in an effort to better protect the skin from the hazards of sun exposure. -
Causes and risk factors of warts
Jan 14, 23 05:02 PM
A good review of the causes of warts and protective measures you can take to prevent developing them. -
Do chronic wounds need to be dressed daily?
Jan 11, 23 02:18 PM
Because of supply chain shortages as well as staffing shortages particularly during the pandemic, many institutions extended the time between dressing changes for chronic wounds. Is this really the be… -
Food choices that raise your risk of type 2 diabetes
Jan 08, 23 10:07 AM
A good review of how blood sugars can become elevated and the harm that can do. Certain food groups have a tendency to raise your blood sugars and should be avoided. -
Outcome stats from Scarf bunionectomy
Jan 03, 23 03:04 PM
The Journal of Foot and Ankle Surgery recently reported a meta analysis of outcomes in 1583 Scarf bunionectomies that met their inclusion criteria. Adverse events did not seem to be any better or wors…